
Shoulder Fractures
Proximal Humeral Fractures
Fractures of the proximal humerus are common, accounting for 5% of all fractures. These fractures tend to occur in older patients who are osteoporotic.
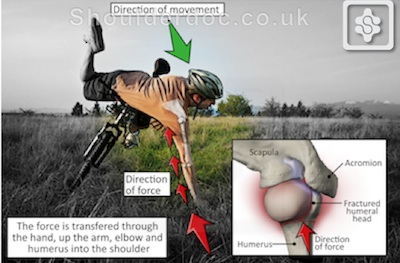
The most common mechanism for these fractures is a fall on the outstretched hand from a standing height. In younger patients, high-energy trauma is the cause of injury.
The treatment objective in proximal humerus fractures is to allow bone and soft tissue healing in a normal anatomical position to maximise function of the upper extremity.
Most fractures are minimally displaced and stable, so surgical fixation is not required. A supportive sling followed by early rehabilitation and have good functional outcomes.
Displaced fractures require reconstuction, because if left untreated will have a high likelihood of producing limited function.
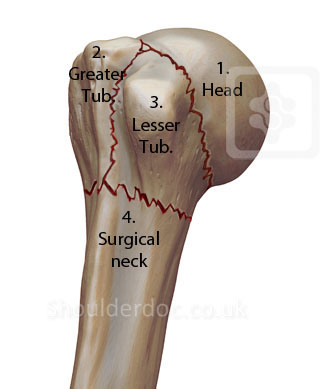
The most common definition of displacement is 1 cm between fragments or 45° of angulation between fracture fragments. The parts that most commonly produce these fragments are the humeral head, the greater and lesser tuberosities, and the surgical neck.
The fracture pattern can be complex and difficult to assess adequately with plain x-rays, so a CT scan may be required to better understand the severity of the fracture.
The decision for surgery and the surgical methods require a skilled and experienced surgeon and a motivated patient. The personality of the fracture (eg, bone quality, fracture orientation, concurrent soft tissue injuries), the personality of the patient (eg, compliant, realistic expectations, mental status), and the personality of the surgeon (eg, surgical experience, technical familiarity, available resources) all have a tremendous effect on specific treatment indications.
Below are two examples of displaced fractures that require surgical fixation:


2 part displaced 3 part displaced
The overall prognosis from proximal humerus fractures depends on numerous factors, including the following:
- Type of fracture (Neer type)
- Age of the patient
- Overall health status of patient
- Patient’s expectations
- Willingness of the patient to undergo lengthy rehabilitation
- Ability to restore stability of the fracture with anatomic restoration in surgically treated fractures
These fractures require at least 1 year for recovery.











