
Elbow Replacement
Total Elbow Replacement
Although elbow joint replacement is much less common than knee or hip replacement, it is just as successful in relieving joint pain and returning people to activities they enjoy.
In 2010, about 3,000 people in the U.S. had elbow replacement surgery, according to the Agency for Healthcare Research and Quality.
Whether you have just begun exploring treatment options or have already decided to have elbow replacement surgery, this article will help you understand more about this valuable procedure.
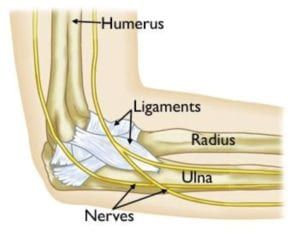
Anatomy
The elbow is a hinge joint which is made up of three bones:
- The humerus (upper arm bone)
- The ulna (forearm bone on the pinky finger side)
- The radius (forearm bone on the thumb side)
The surfaces of the bones where they meet to form the elbow joint are covered with articular cartilage, a smooth substance that protects the bones and enables them to move easily. A thin, smooth tissue called synovial membrane covers all remaining surfaces inside the elbow joint. In a healthy elbow, this membrane makes a small amount of fluid that lubricates the cartilage and eliminates almost any friction as you bend and rotate your arm.
Muscles, ligaments, and tendons hold the elbow joint together.
Description
In total elbow replacement surgery, the damaged parts of the humerus and ulna are replaced with artificial components. The artificial elbow joint is made up of a metal and plastic hinge with two metal stems. The stems fit inside the hollow part of the bone called the canal.
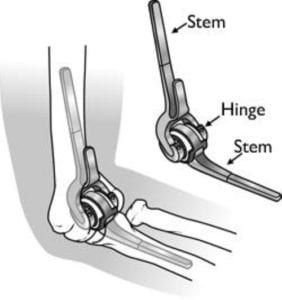
There are different types of elbow replacements, and components come in different sizes. There are also partial elbow replacements, which may be used in very specific situations. A discussion with your doctor will help to determine what type of elbow replacement is best for you.
Several conditions can cause elbow pain and disability, and lead patients and their doctors to consider elbow joint replacement surgery.
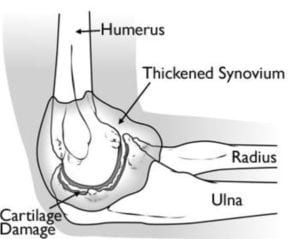
Rheumatoid Arthritis
This is a disease in which the synovial membrane that surrounds the joint becomes inflamed and thickened. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness.
Rheumatoid arthritis is the most common form of a group of disorders termed “inflammatory arthritis.”
Osteoarthritis (Degenerative Joint Disease)
Osteoarthritis is an age-related, “wear and tear” type of arthritis. It usually occurs in people 50 years of age and older, but may occur in younger people, too. The cartilage that cushions the bones of the elbow softens and wears away. The bones then rub against one another. Over time, the elbow joint becomes stiff and painful.
Post-traumatic Arthritis
This type of arthritis can follow a serious elbow injury. Fractures of the bones that make up the elbow, or tears of the surrounding tendons and ligaments may cause damage to the articular cartilage over time. This causes pain and limits elbow function.
Severe Fractures
A severe fracture of one or more bones that make up the elbow is another common reason people have elbow replacements. If the elbow is shattered, it may be very difficult for a doctor to put the pieces of bone back in place. In addition, the blood supply to the bone pieces can be interrupted. In this type of case, a surgeon may recommend an elbow replacement. Older patients with osteoporosis (fragile bone) are most at risk for severe elbow fractures.
In addition, some fractures do not heal well and may require an elbow replacement to address continuing problems.
Instability
Instability occurs when the ligaments that hold the elbow joint together are damaged and do not work well. The elbow is prone to dislocation. Chronic instability is most often caused by an injury.
Medical Evaluation
If you decide to have elbow replacement surgery, your orthopaedic surgeon may ask you to schedule a complete physical examination with your family physician several weeks before surgery. This is needed to make sure you are healthy enough to have the surgery and complete the recovery process.
Many patients with chronic medical conditions, like heart disease, must also be evaluated by a specialist, such a cardiologist, before the surgery.
Medications
Be sure to talk to your orthopaedic surgeon about the medications you take. Some medications may need to be stopped before surgery. For example, the following over-the-counter medicines may cause excessive bleeding and should be stopped 2 weeks before surgery:
- Non-steroidal anti-inflammatory medications, such as aspirin, ibuprofen, and naproxen sodium
- Most arthritis medications
If you take blood thinners, either your primary care doctor or cardiologist will advise you about stopping these medications before surgery.
Home Planning
Making simple changes in your home before surgery can make your recovery period easier.
For the first several weeks after your surgery, it will be hard to reach high shelves and cupboards. Before your surgery, be sure to go through your home and place any items you may need afterwards on low shelves.
When you come home from the hospital, you will need help for a few weeks with some daily tasks like dressing, bathing, cooking, and laundry. If you will not have any support at home immediately after surgery, you may need a short stay in a rehabilitation facility until you become more independent.
Before Your Operation
You will most likely be admitted to the hospital on the day of your surgery. After admission, you will be taken to the preoperative preparation area and will meet a doctor from the anesthesia department.
You, your anesthesiologist, and your surgeon will discuss the type of anesthesia to be used. In most total elbow replacement surgeries, a general anesthetic that puts you to sleep for the entire operation is used.
Surgical Procedure
To reach the elbow joint, your surgeon will make an incision (cut), usually at the back of the elbow. After making the incision, your surgeon will gently move muscles aside to get access to the bone. After removing scar tissue and spurs around the joint, your surgeon will prepare the humerus to fit the metallic piece that will replace that side of the joint. The same preparation is done for the ulna.
The replacement stems are placed into the humerus and ulna bones, and kept in place with a bone cement. The two stems are connected by a hinge pin. After the wound is closed, a padded dressing is then placed to protect the incision while it heals.
Some surgeons will place a temporary tube in the joint to drain the surgical fluid. This tube can be easily removed in your hospital room within the first few days after surgery.

Implants
The metal replacement parts are made of chrome-cobalt alloy or titanium and there is a liner made of polyethylene (plastic). The bone cement is made of polymethylmethacrylate (acrylic, a type of plastic).
Your medical team will give you several doses of antibiotics to prevent infection. Most patients are able to eat solid food and get out of bed the day after surgery. You will most likely stay at the hospital 2 to 4 days after your surgery.
Pain Management
After surgery, you will feel some pain, but your surgeon and nurses will provide medication to make you feel as comfortable as possible. Talk with your surgeon if postoperative pain becomes a problem.
Rehabilitation
A careful, well-planned rehabilitation program is critical to the success of an elbow replacement. You will be taught some exercises for your hand and wrist to avoid stiffness and help to control swelling. You will do gentle elbow range-of-motion exercises as the incision heals. Your doctor may prescribe therapy or may teach you how to do the exercises yourself.
You will most likely not be allowed to put any weight on your arm or push against resistance with your hand until about 6 weeks after your surgery.
Your orthopaedic surgeon will explain the potential risks and complications of elbow joint replacement, including those related to the surgery itself and those that can occur over time after your surgery.
Most complications can be successfully treated. Possible complications are described below.
Infection
Infection is a complication of any surgery. In elbow replacement, infection may occur in the wound or deep around the artificial components. It may happen while in the hospital or after you go home. It may even occur years later. Any infection in your body can spread to your joint replacement.
Minor infections in the wound area are generally treated with antibiotics. Major or deep infections may require more surgery and removal of the components.
Talk to your doctor about obtaining a prescription for antibiotics any time you schedule an invasive procedure, such as surgery or dental procedures. These kinds of procedures cause a temporary spilling of bacteria into your bloodstream which can cause an infection in the replaced joint.
Implant Problems
Although implant designs and materials, as well as surgical techniques, continue to advance, the implant may wear down and the components may loosen. The plastic liner (called the bushings) can wear out, and may need to be replaced. Excessive wear, loosening, or implant breakage may require additional surgery (called a revision procedure).
Nerve Injury
Nerves in the vicinity of the joint replacement may be damaged during surgery, although this type of injury is infrequent. Over time, these nerve injuries typically improve without needing treatment.
Wound Healing
It is important to carefully protect your incision to avoid wound healing problems.
The majority of patients have experienced an improved quality of life after total elbow replacement surgery. They experience less pain, improved motion and strength, and better function.
You should expect to do all basic activities of daily living, such as getting a plate out of a cabinet, cooking dinner, lifting a milk jug, styling your hair, basic hygiene, and dressing. Talk to your doctor about activities you may want to avoid, such as contact sports and activities with a major risk of falling (such as horseback riding or climbing ladders), as well as heavy lifting. These things increase the risk of the metal parts loosening or breaking, or the bone breaking.
When traveling on airplanes, be prepared for extra security screening. There is a chance that your metal implant will set off the metal detector during the security check-in.
To make the check-in go more smoothly, tell the security officer beforehand that you have an elbow replacement and carry a medical identification card. Although this does not change the screening requirements, it will help the security officer confirm the nature of the alarm. Be prepared for the security officer to use a wand scanner, and perhaps examine your arm in a private area in order to see the scar. The new body scanners can identify joint replacements, making further individual screening unnecessary.
Research is being done in the area of implant design in order to make the replacement components last as long as possible.
Because total elbow replacements are often needed by people with rheumatoid arthritis, a lot of research is conducted into joint degeneration in these patients. Many newer medications are available that help to slow down the disease and often avoid the need for an elbow replacement. There is no medication, however, that will turn back time and restore the elbow to normal once the disease has progressed.











